
The Legacy of Black Birthwork

A Legacy That Never Disappeared
Black birthwork exists within a long lineage of care shaped by community, memory, and survival.
Long before care was centralized within medical institutions, midwives held knowledge that lived in practice, in relationship, and in everyday life. That knowledge moved through generations, carried forward across the Black diaspora and adapted to the conditions people were living through.
For centuries, Black midwives have served as healers, caretakers, and advocates within their communities. Their work has never been limited to labor and delivery. It has included pregnancy, postpartum recovery, family care, and the broader realities that shape health and wellbeing.
Much of this care existed outside of formal systems, and often in spite of them.
That lineage continues to shape how care is practiced today, even when it is not always named or recognized.
Collection of the Smithsonian National Museum of African American History and Culture.
Gift of Robert Galbraith. © 1987 Robert Galbraith.
Birth as Cultural, Spiritual, and Communal
In many West African traditions, birth was never treated as an isolated medical event.
It was relational.
It was spiritual.
It was held within community.
Midwives carried knowledge of the body, but also of ritual, land, and connection. They worked with herbal medicine, hands-on techniques, and spiritual practices that supported both the birthing person and the people around them.
Across the diaspora, these practices adapted but remained connected. In the United States, they lived on through granny midwives. In Latin America, through parteras and comadronas. The names shifted. The roots did not.

What Was Carried Through Enslavement
During the transatlantic slave trade, Black women carried knowledge of birth and healing with them, even as nearly every other form of autonomy was taken.
Midwives continued to care for pregnant people, newborns, and families under conditions shaped by violence, displacement, and control. They supported births among enslaved people and were often required and forced to attend births and breastfeed for slaveholding families and their babies as well.
Their work moved across plantations and regions, forming quiet networks of care that held communities together in ways that were not always visible, but deeply felt.
This knowledge lived in practice, in memory, and in relationship. It was shaped by what people were surviving, and by the responsibility to care for one another within those conditions.

The Role of Granny Midwives
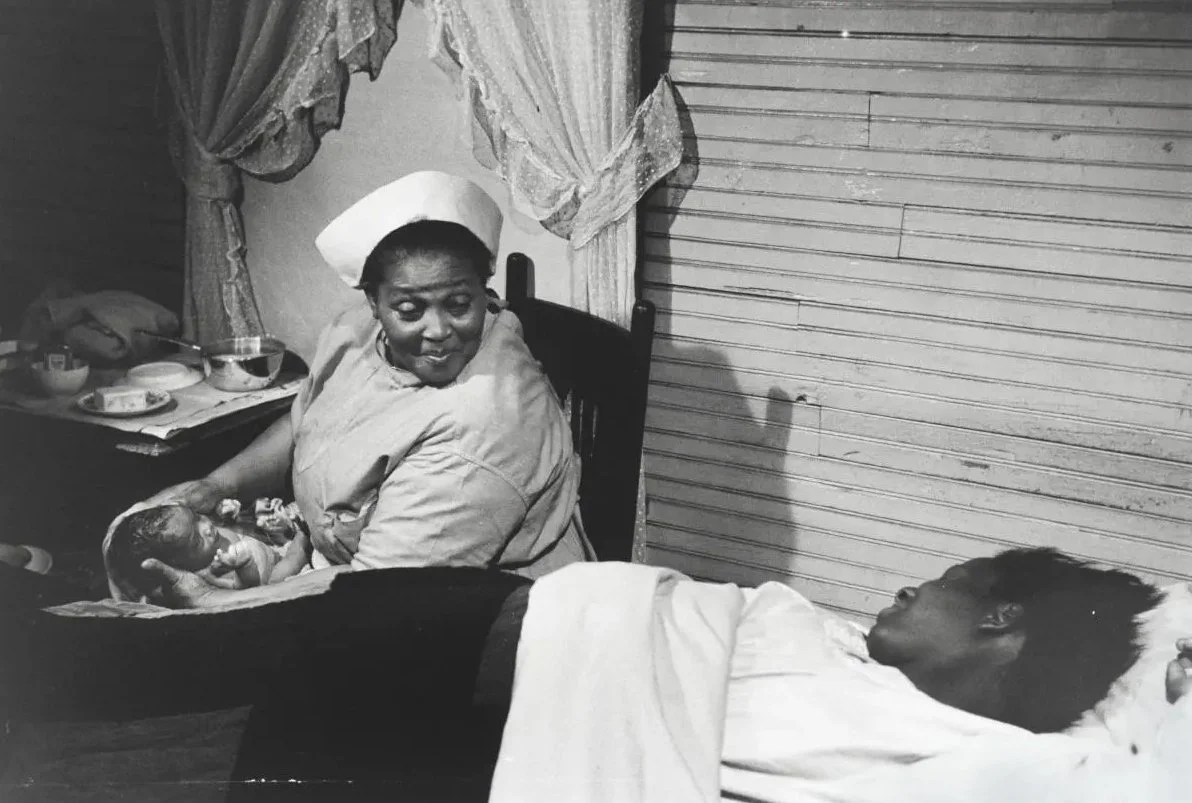
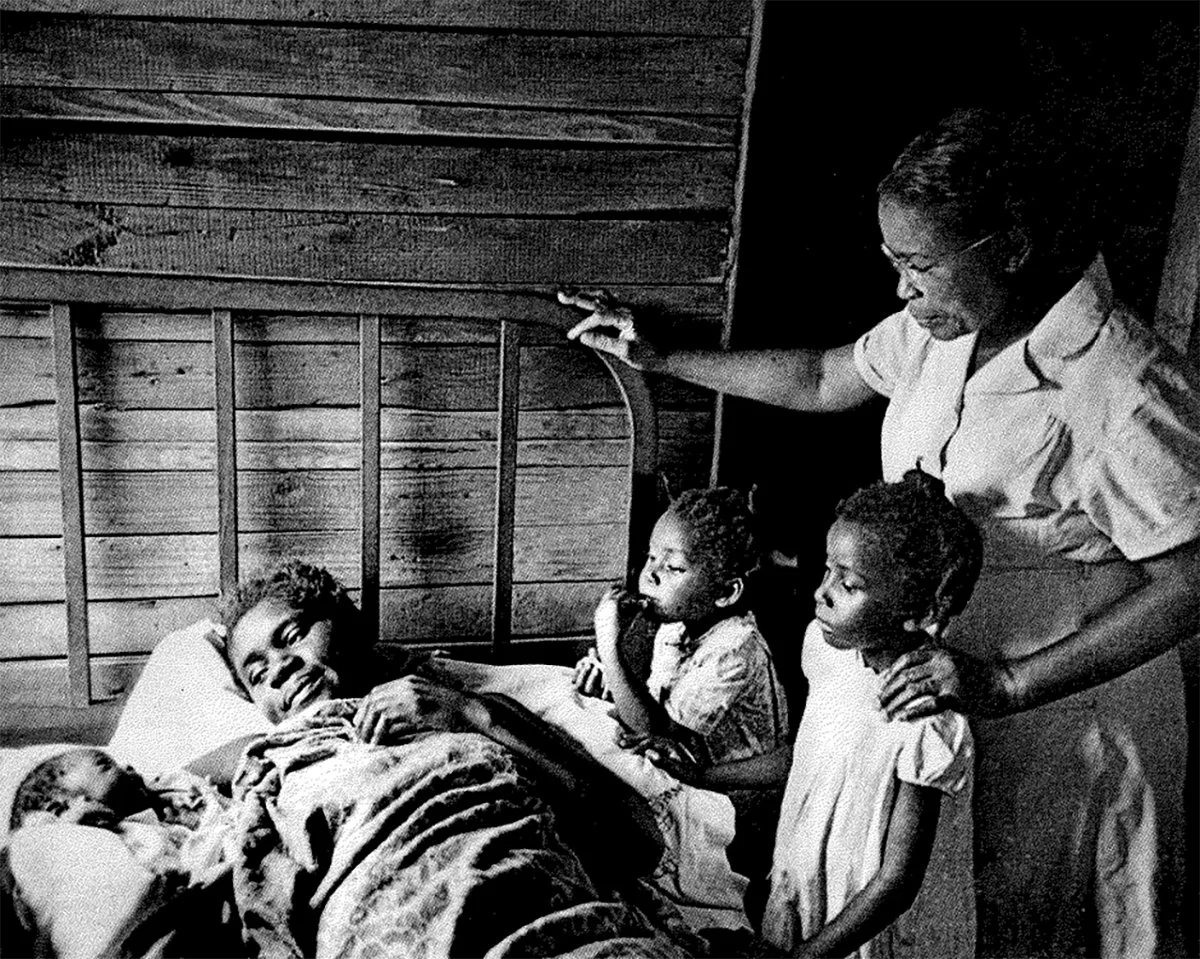
After emancipation, Black midwives remained central to maternal care, especially across the rural South.
Often referred to as granny midwives, they were trusted figures who supported families regardless of income, geography, or access to formal healthcare.
They did far more than attend births.
They provided prenatal guidance.
They supported postpartum healing.
They offered breastfeeding support, nutrition education, and family care.
They were part of the fabric of everyday life.
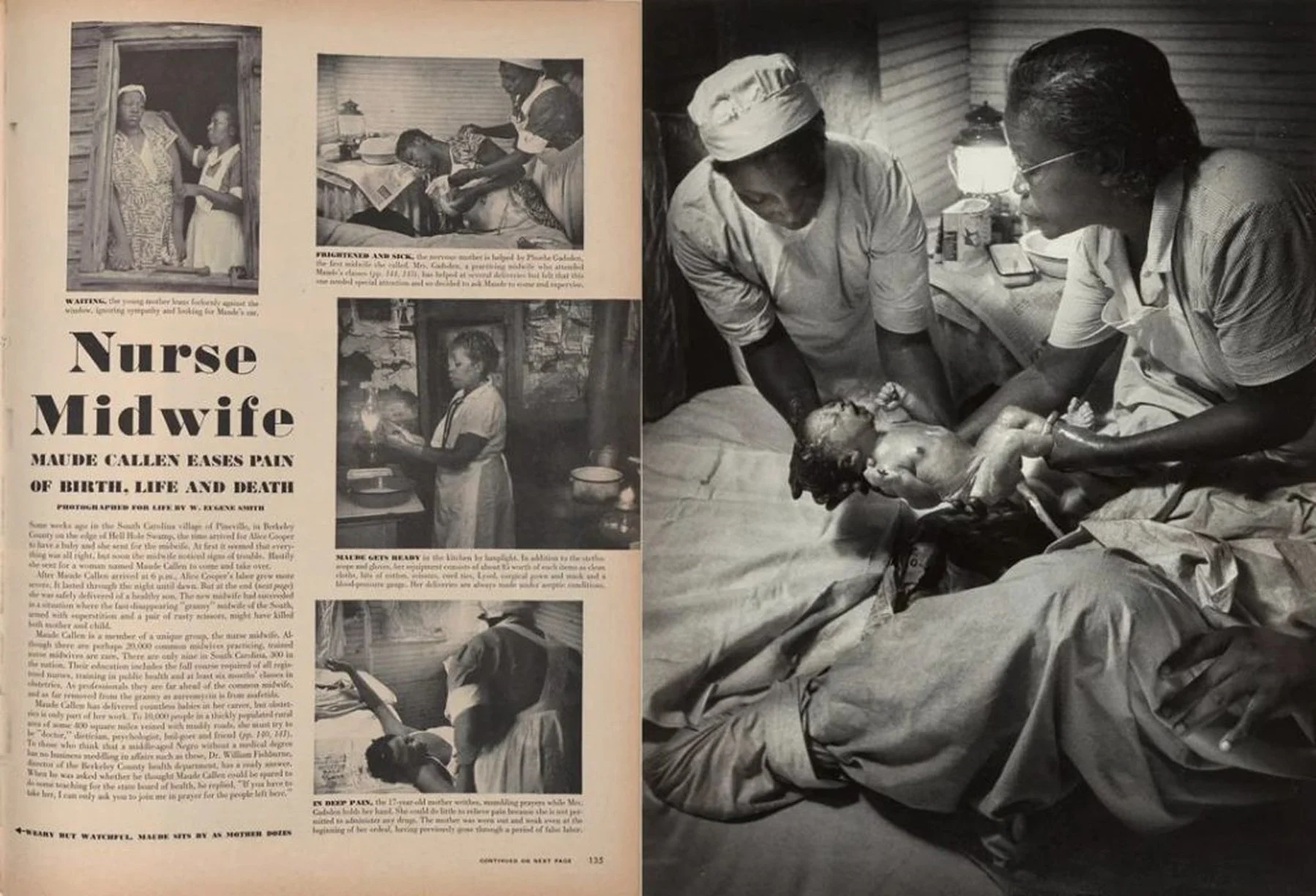
By the early 20th century, midwives were still attending a significant percentage of births in the United States, particularly within Black communities.

Midwife Mary Francis Hill Coley at home, pictured with photos of the 3,000 children she helped bring into the world. Still from All My Babies (1953).

© Time & Life Pictures/Getty Images
Artifacts and photos honoring Black midwives in rural DeSoto County and the Mid-South, on display at the DeSoto County Museum for Black History Month.
The Systematic Pushout
The role of Black midwives began to narrow as childbirth moved further into formal medical institutions.
As obstetrics expanded, new regulations and licensing systems reshaped who was allowed to provide care. Public health campaigns and medical narratives increasingly positioned Black midwives as untrained or unsafe, despite the depth of their experience and the trust they held within their communities.
These shifts were not neutral. They unfolded within a broader context of racism, gendered power, and a growing emphasis on centralized medical authority.
By the mid-20th century, traditional midwifery had been significantly reduced across much of the United States.
Along with it, something harder to measure was also diminished. Care that had been continuous, relational, and grounded in cultural understanding became more fragmented and less connected to the communities it once served.

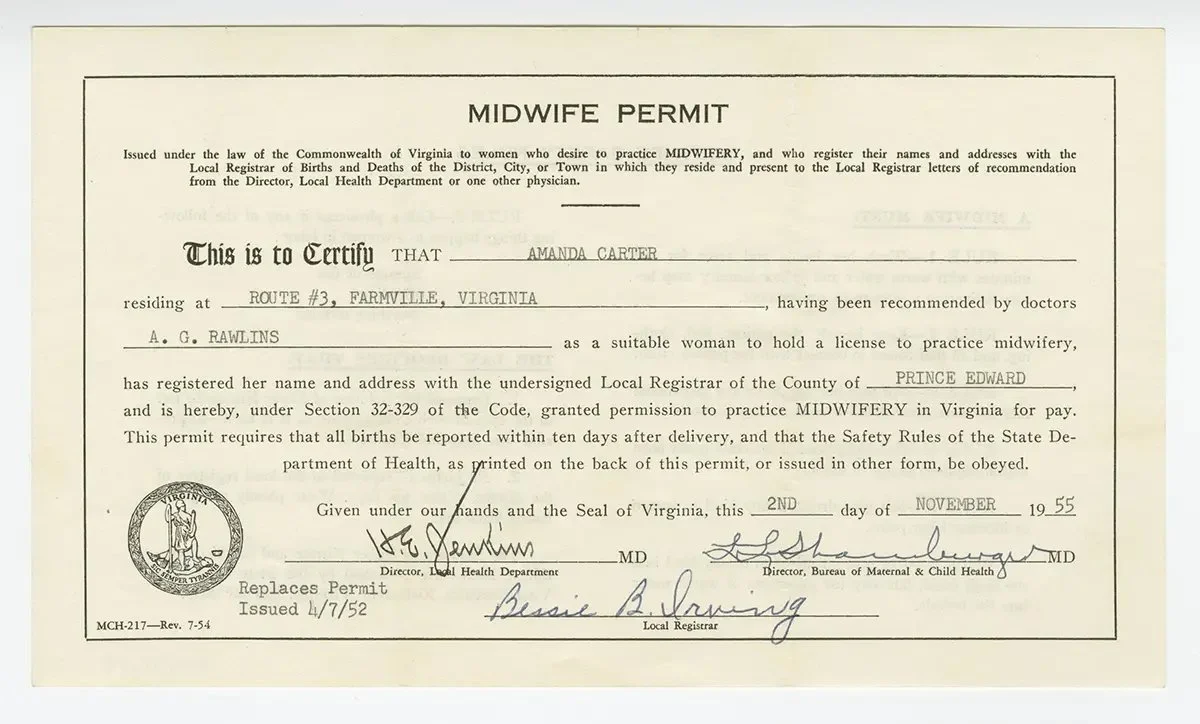
Midwife permit issued to Amanda Carey Carter, November 2, 1955, by the Virginia Department of Health—certifying and regulating birthworkers under state standards.
Collection of the Smithsonian National Museum of African American History and Culture. Gift of Fannie Mae Carter Silver.

Still from All My Babies (1987), featuring midwife Mary Francis Hill Coley (center) with colleagues during hospital training.
Collection of the Smithsonian National Museum of African American History and Culture. Gift of Robert Galbraith. © 1987 Robert Galbraith
What That Loss Created
The impact of that displacement is still visible.
Black women are three to four times more likely to die from pregnancy-related causes than white women in the United States.
These outcomes are shaped by systemic inequities, including unequal access to care, bias within medical systems, and the long-term effects of structural racism.
Care became more clinical, but not necessarily more equitable.
For many Black birthing people, safety within healthcare settings is still not guaranteed.
The Work That Continues
Black birthwork has never disappeared.
Midwives, doulas, and other birthworkers continue to carry forward practices grounded in dignity, autonomy, and whole-person care.
Doulas provide emotional, physical, and advocacy-based support.
Midwives offer clinical care rooted in a holistic understanding of pregnancy and birth.
Together, they create conditions where people feel supported, informed, and respected.
Research continues to show that midwifery-led and community-based care improves outcomes, including lower intervention rates and better maternal and infant health.

Debbie Allen, LM, CPM, founder of Tribe Midwifery, providing care to a patient in her home.
What Is Shifting Now
Midwifery is in the middle of another shift.
Across the country, many training programs are moving toward requiring a doctoral degree, such as a Doctor of Nursing Practice or Doctor of Midwifery, for entry-level certified nurse-midwives. Some institutions describe this as preparation for leadership within increasingly complex healthcare systems.
At the same time, there is ongoing conversation within the field about what this shift changes in practice, and who it makes the profession more or less accessible to.
The American College of Nurse-Midwives has stated that there is no clear evidence that a clinical doctorate leads to better patient outcomes. What has changed more visibly is the cost of training and the amount of time it takes to enter the profession.
Those changes carry different weight depending on who is trying to enter the field.
Black, Indigenous, and other practitioners of color remain underrepresented in midwifery today, even though Black midwives once provided the majority of care in many communities.
As educational requirements expand, questions around access become harder to ignore. Tuition, time, and institutional pathways all shape who is able to train, who is able to stay, and who is able to practice.
There is also a quieter tension underneath these changes.
Midwifery has long been shaped by knowledge that lives outside of formal institutions, passed through apprenticeship, community practice, and lived experience. As the profession becomes more standardized, there is an ongoing negotiation between formal credentials and the forms of expertise that have always sustained this work.
All of this shapes who is able to enter the field, who remains in it, and who is reflected within it.
That question carries weight, especially when the communities most impacted by maternal health inequities are often the least represented within the systems meant to care for them.
What It Means to Restore Birth Justice
Improving maternal health calls for a deeper look at how care is defined, practiced, and resourced.
It also asks us to recognize the knowledge systems that have been pushed aside, and how their absence continues to shape care today.
Across the Black diaspora, traditional midwifery has long held a different orientation toward care. One that centers:
Community involvement
Cultural understanding
Continuity of care
Respect for the birthing person
These approaches have never been peripheral. They have shaped how care is experienced, how trust is built, and how people move through pregnancy and birth.
Restoring birth justice means creating the conditions where this kind of care can exist fully supported, recognized, and accessible to the communities who have always carried it forward.
Our Commitment
At Lyon-Martin, we understand that healthcare is shaped by history, by policy, and by lived experience.
We are committed to care that is trauma-informed, culturally responsive, and grounded in dignity and self-determination.
Honoring the legacy of Black birthwork means supporting models of care that center community, trust, and autonomy.
It also means continuing to examine and challenge the systems that have created inequities in the first place.

This Black Maternal Health Week
This week offers space to honor the generations of Black midwives and birthworkers whose knowledge has carried communities through conditions that were never designed for their survival.
It also brings attention to what remains unresolved. The gaps in care, the inequities in outcomes, and the ongoing need for systems that can actually hold people with dignity and respect.
Black birthwork has always been rooted in relationship, in accountability to community, and in a deep understanding of what it means to care for someone through one of the most vulnerable moments in their life.
That knowledge is still here, practiced every day in homes, clinics, and communities.
What happens next depends on whether the systems shaping care are willing to recognize what has always been here, and to trust the communities who have been carrying it forward.
Sources:
CDC, Maternal Mortality Rates in the United States, 2024
https://www.cdc.gov/nchs/data/hestat/hestat113.htm
CDC, Working Together to Reduce Black Maternal Mortality
https://www.cdc.gov/womens-health/features/maternal-mortality.html
The Training of African American Traditional Midwives, 1920–1940
https://pmc.ncbi.nlm.nih.gov/articles/PMC2804652/
National Museum of African American History and Culture, African Americans at Work: A Photo Essay
https://nmaahc.si.edu/explore/stories/african-americans-at-work
Cochrane Review, Midwife continuity of care models versus other models of care for childbearing women (2024)
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004667.pub6/pdf/full/en
WHO, Midwifery page
https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/maternal-health/midwifery
Doula care across the maternity care continuum and impact on maternal health: a scoping review
https://pmc.ncbi.nlm.nih.gov/articles/PMC9257331/
Impact of Doulas on Healthy Birth Outcomes
https://pmc.ncbi.nlm.nih.gov/articles/PMC3647727/
ACNM, Midwifery Education and Doctoral Preparation (2025)
https://midwife.org/wp-content/uploads/2025/12/2025-ps_midwifery-education_doctoral_preparation.pdf
AACN, DNP Education
https://www.aacnnursing.org/students/nursing-education-pathways/dnp-education
ACNM, Position Statement
https://midwife.org/wp-content/uploads/2025/02/Certified-Nurse-Midwife-and-Certified-Midwife-Education-and-Certification-in-the-United-States.pdf
ACNM, Truth and Reconciliation Resolution
https://midwife.org/wp-content/uploads/2024/09/ACNM_Truth_and_Reconciliation_Resolution-Apr2021.pdf
UCSF Favors Pricey Doctoral Program for Nurse-Midwives Amid Maternal Care Crisis
https://www.chcf.org/resource/ucsf-favors-pricey-doctoral-program-nurse-midwives-amid-maternal-care-crisis/
Doctor of nursing practice (DNP) degree in the United States: Reflecting, readjusting, and getting back on track
https://pmc.ncbi.nlm.nih.gov/articles/PMC7161484/